


Cancer Targets
Target Search
Background
What is Cancer?
At its core, cancer (tumor) is the result of uncontrolled cell growth. Our bodies are made up of trillions of cells, all working together. In a tumor, one of those cells stops responding to the normal signals that instruct the cell to grow, to grow, and even to die. Cancer cells still have many of the same needs and characteristics as normal cells, but they become less dependent on the controls that keep our bodies functioning smoothly. The process by which normal cells change to behave so abnormally takes a long time and is often triggered by external influences. The following paragraphs describe the difference between normal cells and cancer cells and outline the steps by which normal cells become cancer cells.
Cancer is actually a general term used to describe a large group of related diseases. Each type of cancer is unique, with its own genetic changes and growth characteristics. Some tumors grow rapidly while others take many years to become a threat to patients. These differences between different cancer types (even different types on the same organ, such as different types of breast cancer) are one of the main reasons why cancer treatment is so difficult.
In addition to the differences between different cancer types, all cancer types do share some characteristics, and these common characteristics are the basis of cancer treatment and research. It is important to understand the basic, common features of cancer. This gives us options for studying how to detect, diagnose and treat.
Kinds of Cancer
Cancers can be classified according to their function or location of origin. The following are common names for cancers classified according to their tissue origin.
Malignant epithelial tumors: tumors derived from epithelial cells (cells on the skin and on the surface of various organs). Our digestive tract and organs are also lined with epithelial cells. This is the most common type of cancer, accounting for 80-90% of all reported cancer cases.
Malignant mesenchymal tumors: tumors of muscle, bone, cartilage, fat, or connective tissue.
Leukemia: Cancer of white blood cells or their precursors. The cells that can form both white and blood cells are located in the bone marrow.
Lymphoma: Cells from the bone marrow affect the formation of the lymphatic system.
Myeloma: Formation of white blood cells (B lymphocytes or B cells) responsible for producing antibodies.
Cancer is a leading cause of death worldwide, causing nearly 10 million (or nearly one in six) deaths in 2020. According to WHO data, in 2020, the most common (in terms of new cases of cancer) is breast cancer (2.26 million cases); Lung cancer (2.21 million cases); Colon and rectal cancer (1.93 million cases); Prostate cancer (1.41 million cases); Skin cancer (non-melanoma) (1.2 million cases); Stomach cancer (1.09 million cases).

Breast Cancer: Among the new cases diagnosed, breast cancer is one of the leading cancer types and the most common cause of cancer death in women. In 2017, the American Cancer Society estimates that about 252,710 new cases of breast cancer will be diagnosed. Although fairly rare, it is worth noting that men can also develop breast cancer. Approximately 2,470 of the estimated breast cancer deaths in 2016 will be among men.
Lung Cancer: Lung cancer is currently the leading cause of cancer-related death in both men and women. Although men continued to decline, the incidence in women remained stable. Trends in lung cancer-related deaths mirror trends in smoking over the past few decades.
Colon and Rectal Cancer: Colon and rectal cancer, collectively known as colorectal cancer, share many similar characteristics. Colorectal cancer is currently the third most common cancer in both men and women. Morbidity and mortality rates have been declining since 1980, in part due to improvements in screening and prevention.
Prostate Cancer: Prostate cancer is the most common type of cancer that threatens the lives of men worldwide for millions of years. In the early 1990s, the incidence of prostate cancer increased dramatically. This trend may be related to the development of prostate cancer screening and detection techniques. However, since 2006 the incidence has declined, with about 60,000 fewer cases being diagnosed. The death rate from prostate cancer, on the other hand, did not change. Prostate cancer is the most commonly diagnosed type of cancer in men after skin cancer and is the second leading cause of cancer death in men.
Skin Cancer: Cutaneous malignancies are the most commonly diagnosed cancer type in the world and show a tendency of younger onset. Skin cancer can be classified as non-melanoma skin cancer (cancer types include squamous cell carcinoma and basal cell carcinoma) and melanoma. The most common type of skin cancer is basal cell carcinoma. However, melanoma, which accounts for only 4% of skin cancers, is responsible for 80% of skin cancer deaths.
Stomach Cancer: Stomach cancer is relatively rare in the United States and other developed countries. Although stomach cancer is rare in the United States, it is the second leading cause of cancer-related death worldwide and the fourth most common cancer worldwide. Due to improvements in living conditions and diet, the incidence of most types of stomach cancer is decreasing worldwide.
Liver Cancer: Since the early 1880s, the number of liver cancer patients in the United States has steadily increased. Liver cancer is the seventh most common cancer in women and the fifth most common cancer in men. Europe, Australia and the United States have the highest rates of liver cancer in the world. At present, the prediction of liver cancer is difficult because most cases of liver cancer cannot be detected at an early stage.
Cervical Cancer: Cervical cancer forms in the lining of the cervix, at the junction of the vagina and uterus, and the progression of cervical cancer is usually slow and lasts for years. The progression of cervical cancer begins with the development of precancerous lesions in normal cells. Most of these changes, even if left untreated, will not develop into cancer. Cervical cancer is most often diagnosed in middle-aged women, half of whom are diagnosed between the ages of 35 and 55. Cervical cancer is rarely seen in women under the age of 20, but about 20% of cases occur in women over the age of 65, indicating a need for continued screening. The 5-year survival rate for invasive cervical cancer is now 67 percent, and improvements in screening and the development of preventive vaccines have reduced the incidence of advanced cancers.
Symptoms of Cancer

Pain: Many cancers are generally painless at first, but pain can be an early symptom of some cancers, such as headaches caused by brain tumors and painful swallowing caused by head and neck cancer and esophageal cancer. As the cancer grows, the initial symptoms are often mild discomfort, which can escalate into more and more severe pain as the cancer expands. Pain may be caused by cancer pressing on or eroding nerves or other structures. However, not all cancers cause severe pain. Similarly, the absence of pain does not guarantee that the cancer will not grow or spread.
Hemorrhage: At first, the cancer may bleed slightly because of its weak blood vessels. Later, as the cancer expands and invades surrounding tissue, it may grow into nearby blood vessels, causing bleeding. Bleeding may be slight and undetectable or only detectable during examination. This is often the case in early colon cancer. Or, especially for advanced cancers, bleeding may be more pronounced, even massive and life-threatening.
The site of the cancer determines the site of the bleeding. Cancer anywhere along the digestive tract may cause blood in the stool. Cancer anywhere along the urinary tract may cause blood in the urine. Other cancers may bleed in internal areas of the body. Bleeding in the lungs can cause an individual to cough up blood.
Thrombus: Certain cancers produce substances that cause excessive clotting, mainly in the veins of the lower extremities (deep vein thrombosis). Blood clots in lower limb veins sometimes break off and travel to the lungs (pulmonary embolism), which can be fatal. Excessive clotting is common in patients with pancreatic, lung, and other solid tumors, as well as in patients with brain tumors.
Weight Loss and Fatigue: Often, cancer patients experience weight loss and fatigue, which can worsen as the cancer progresses. Despite the good appetite, some people notice weight loss. Others have decreased appetite and may even experience food nausea or difficulty swallowing. They may become very thin. Patients with advanced cancer are often very tired. If anemia occurs, these patients may find themselves feeling tired or short of breath even with light activity.
Lymphadenopathy: When cancer begins to spread in the body, it may first spread to nearby lymph nodes, causing them to become swollen. Swollen lymph nodes are usually painless, and they may feel hard or pliable to the touch. They may be well mobile, or if the cancer is more advanced, they may stick to the surrounding tissue or to each other.
Neurological Symptoms and Muscular Symptoms: Cancer can grow into or press on the nerves or spinal cord, causing any of several neurological and muscular symptoms, including pain, weakness, or sensory changes (such as tingling sensations). When cancer is growing in the brain, symptoms can be difficult to determine, but can include confusion, dizziness, headache, nausea, vision changes, and seizures. Neurological symptoms can also be part of paraneoplastic syndromes.
Respiratory Symptoms: Cancer can compress or block the airways in the lungs, leading to shortness of breath, coughing or pneumonia. Shortness of breath may also occur when the cancer causes a large pleural effusion, bleeding in the lungs, or anemia.
Causes of Cancer

Genetic Risk
The occurrence of some cancers is a family history. Some families have a significantly higher risk of certain cancers. Sometimes it's due to a single gene, and sometimes it's due to multiple genes interacting. Genetic mutations that cause cancer can be caused by the damaging effects of chemicals, sunlight, drugs, viruses or other environmental substances. In some families, these abnormal oncogenes are inherited.
Environmental Risk
Tobacco smoke contains a number of carcinogens that significantly increase the risk of developing cancers of the lung, mouth, throat, esophagus, kidney and bladder.
Pollutants in the air or water, such as asbestos, industrial waste or tobacco smoke, can increase cancer risk. Many chemicals are known to cause cancer, while some are suspected of causing cancer. For example, exposure to asbestos can lead to lung cancer and mesothelioma (cancer of the pleura). Pesticide exposure is associated with an increased risk of certain types of cancer, such as leukemia and non-Hodgkin's lymphoma.
Exposure to radiation is a risk factor for developing cancer. Excessive exposure to ultraviolet light (mainly sunlight) can lead to skin cancer.
Exposure to radon, a radioactive gas released from the soil, increases the risk of lung cancer. Usually, radon quickly dissipates harmlessly into the atmosphere. However, when buildings are built on land with high radon levels, radon can accumulate inside your building and sometimes produce high enough levels of radon in the air to cause harm.
Biological Risk
Several viruses are known to cause cancer in humans, while several are suspected of causing cancer. Human papillomavirus (HPV, which causes genital warts) is the leading cause of cervical and vulvar cancers in women and penile and anal cancers in men. HPV also causes some cancers of the mouth and throat. Hepatitis B virus or hepatitis C virus can cause liver cancer. Some human retroviruses, such as HIV, can cause lymphoma and other cancers of the blood system. Helicobacter pylori, which causes stomach ulcers, can increase the risk of stomach cancer and lymphoma.
Inflammatory diseases often increase the risk of cancer. Such diseases include ulcerative colitis and Crohn's disease (which can lead to colon and bile duct cancer).
Therapeutic of Cancer

The treatment given to cancer is variable and depends on many factors, including the type, location and number of diseases and the patient's health status. Most treatments either kill/remove cancer cells directly or cause them to eventually die by depriving them of the signals they need to survive. Other therapies work by stimulating the body's own defenses against cancer cells.
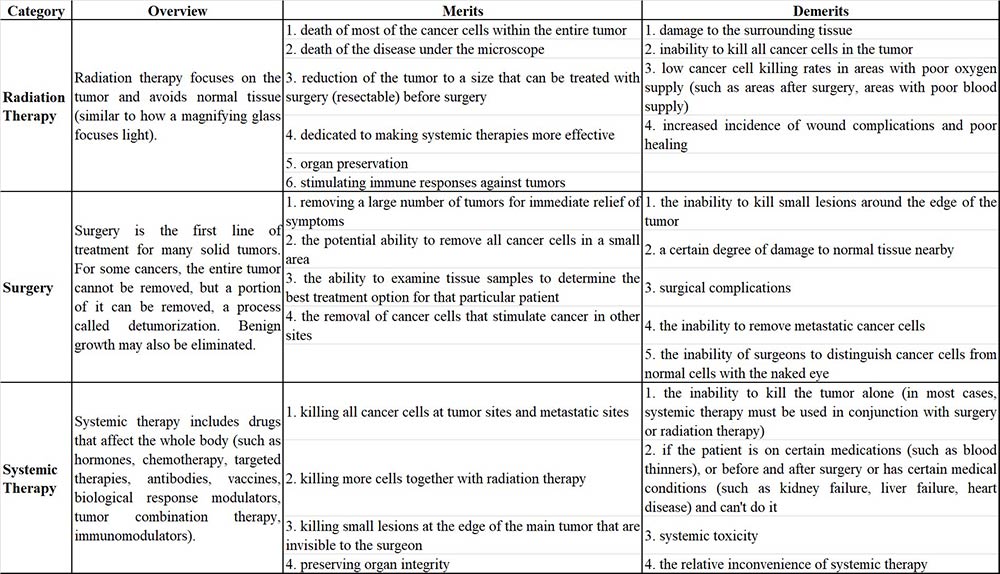
There are three general types of cancer treatments, including: Radiation therapy (provided by a radiation oncologist); Surgery (performed by a surgical oncologist); Systemic therapy (usually administered by a medical oncologist). The goal of any treatment is to kill as many cancer cells as possible and minimize the death of normal cells. Each type of treatment has advantages and disadvantages. In most cancers, multiple treatment regimens must be used together (simultaneously or one after the other) to get the best results.
Case Study
Case Study 1: Recombinant Human AXL protein(Met1-Pro449) (AXL-769H)
Aptamers, synthetic single-strand oligonucleotides that are similar in function to antibodies, are promising as therapeutics because of their minimal side effects. However, the stability and bioavailability of the aptamers pose a challenge. The researchers developed aptamers converted from RNA aptamer to modified DNA aptamers that target phospho-AXL with improved stability and bioavailability. On the basis of the comparative analysis of a library of 17 converted modified DNA aptamers, they selected aptamer candidates, GLB-G25 and GLB-A04, that exhibited the highest bioavailability, stability, and robust antitumor effect in in vitro experiments. Microscale Thermophoresis experiments were performed in buffers containing recombinant AXL proteins to evaluate the binding capacity of GLB-G25 and GLB-A04.Backbone modifications such as thiophosphate or dithiophosphate and a covalent modification of the 5'-end of the aptamer with polyethylene glycol optimized the pharmacokinetic properties, improved the stability of the aptamers in vivo by reducing nuclease hydrolysis and renal clearance, and achieved high and sustained inhibition of AXL at a very low dose.
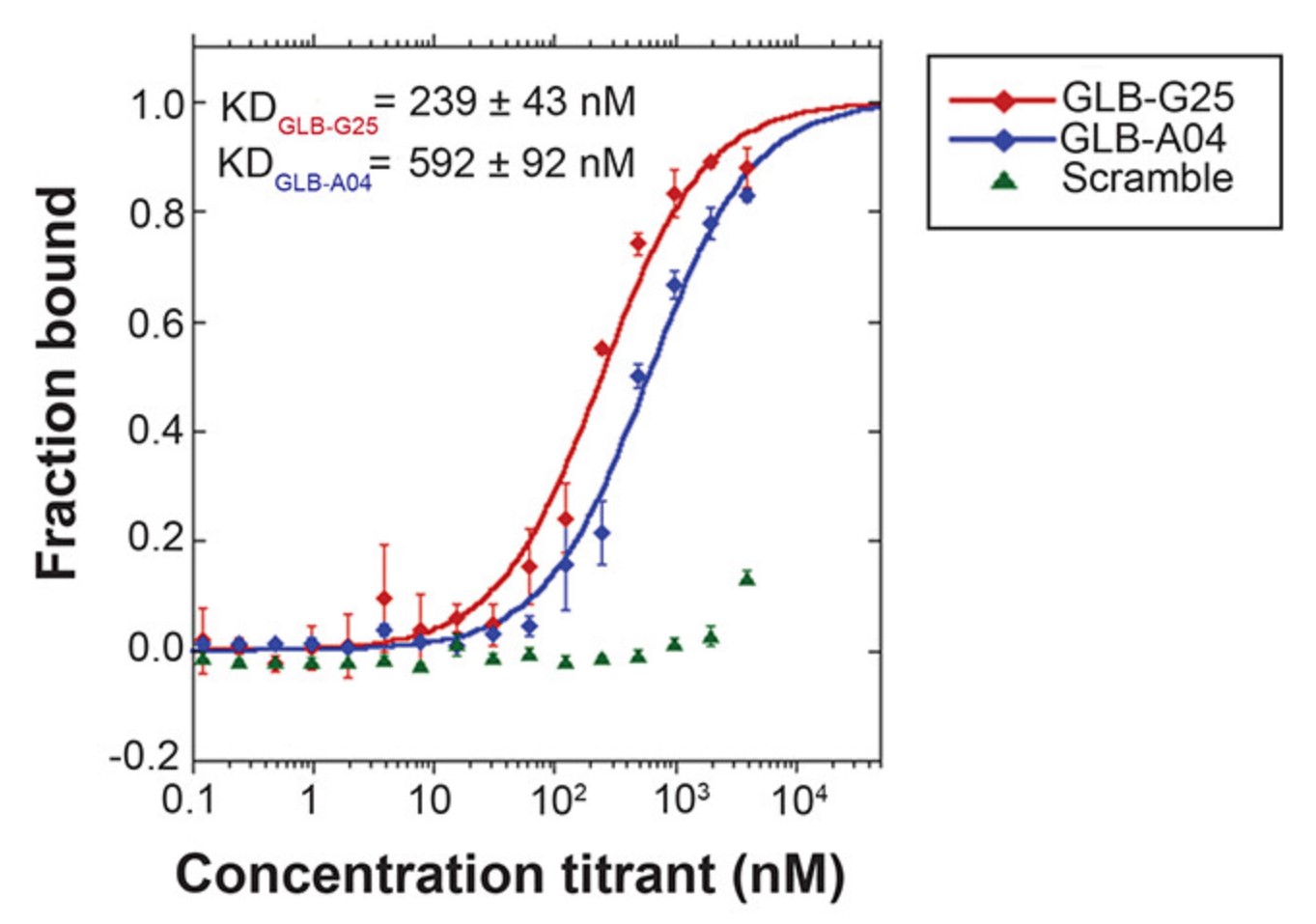
Fig1. GLB-G25 and GLB-A04 binding curve obtained by MicroScale Thermophoresis (MST). (Paola Amero, 2021)
Case Study 2: Recombinant Human CASP3 (CASP3-158H)
Proteolytic truncation of microtubule-associated human (h) Tau proteins by caspase-3 at the carboxyl (C) end has been implicated in the pathogenesis of Alzheimer's disease (AD). This cleavage can occur between Asp421-Ser422, resulting in the formation of 421-mer truncated Tau proteins. It was further suggested that the presence of Ser422 residues at P1' in the hTau caspase-3 cleavage region was a potential phosphorylation site. The goal of the project was to study the caspase-3 cleavage site of hTau protein in vitro and examine the kinetics of this cleavage after Ser422 phosphorylation and treatment with caspase-3 inhibitors. This was achieved by designing a peptide containing the hTau protein sequence of the Caspase-3-cut region. The peptide was designed based on the 441-mer main sequence of human Tau protein, which contains the proposed caspase-3 cleavage site [Asp421-Ser422]. Corresponding phosphoric acid, dextroSER422 and dextroasp421 analogues were designed. The peptides were synthesized and purified by solid phase chemistry and characterized by mass spectrometry. The results showed that when the control peptide was effectively cut by caspase-3 at Asp421-Ser422, the expected N-terminal and C-terminal fragments of peptide were produced, and the corresponding phospho-Ser422 peptide remained completely resistant to cutting. The substitution of Asp421 by its right-handed isomer also blocks the cleavage of the peptide by caspase-3. However, the substitution of Ser422 by its right-handed isomer in the polypeptide did not significantly affect cleavage.
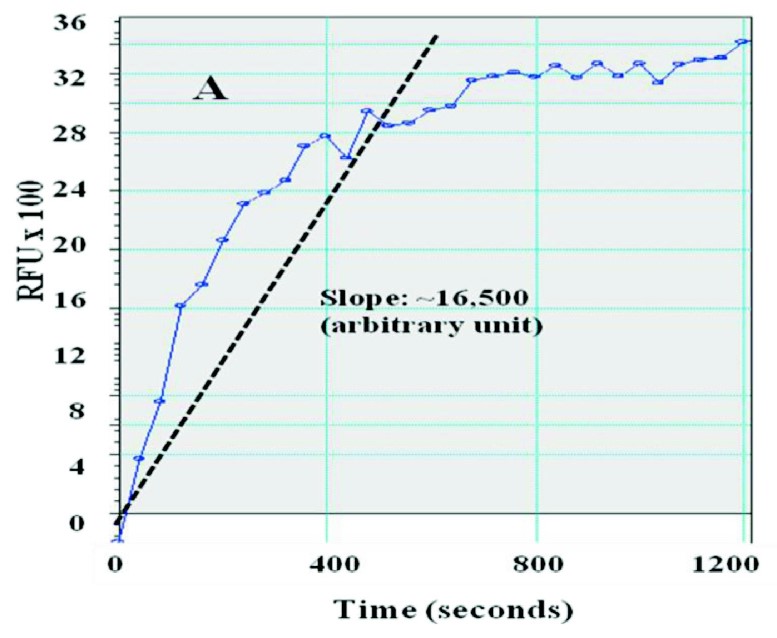
Fig2. In vitro caspase-3 activity assay without inhibitor. (Priya Sandhu, 2017)
Case Study 3: Recombinant Human CD47 protein(Gln19-Pro139) (CD47-7862H)
Nanocarriers (NCs) help improve the performance of therapeutics, but their removal by phagocytes in the liver, spleen, tissues, etc. diminishes this potential. Although NC functionalization with polyethylene glycol (PEG) lowers interaction with phagocytes, it also reduces interactions with tissue cells. Coating NCs with CD47, a protein expressed by body cells to avoid phagocytic removal, offers an alternative. Previous studies showed that coating CD47 on non-targeted NCs reduces phagocytosis, but whether this alters binding and endocytosis of actively-targeted NCs remains unknown. To evaluate this, the researchers used polymer NCs targeted to ICAM-1, a receptor overexpressed in many diseases. Co-coating of CD47 on anti-ICAM NCs reduced macrophage phagocytosis by ∼50% for up to 24 h, while increasing endothelial-cell targeting by ∼87% over control anti-ICAM/IgG NCs. Anti-ICAM/CD47 NCs were endocytosed via the CAM-mediated pathway with efficiency similar (0.99-fold) to anti-ICAM/IgG NCs. Comparable outcomes were observed for NCs targeted to PECAM-1 or transferrin receptor, suggesting broad applicability.
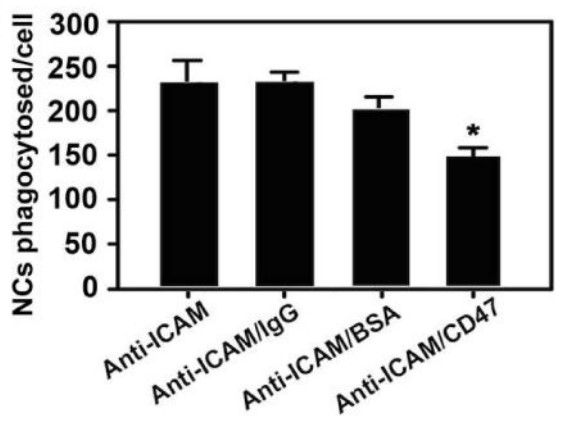
Fig3. Quantification of the uptake of 200 nm diameter model NCs consisting of green fluorescent polystyrene nanoparticles. (Joshua Kim, 2017)
Related Resources
Cancer is a complex and diverse group of diseases that pose significant physical, emotional, and economic burdens to individuals, families, communities, and health systems. The global burden of cancer is increasing, with low- and middle-income countries often being ill-prepared to manage this burden, resulting in many patients not receiving timely and high-quality diagnosis and treatment. Many cancers can be cured if they are detected early and treated effectively.
Contact us or send an email at for project quotations and more detailed information.
Quick Links
-

Papers’ PMID to Obtain Coupon
Submit Now -

Refer Friends & New Lab Start-up Promotions